Hearing and Quality-of-Life Outcomes After Cochlear Implantation in Adult Hearing Aid Users 65 Years or Older
A Secondary Analysis of a Nonrandomized Clinical Trial
Wick CC, Kallogjeri D, McJunkin JL, et al
Assessment of Cochlear Implants for Adult Medicare Beneficiaries Aged 65 Years or Older Who Meet Expanded Indications of Open-Set Sentence Recognition
A Multicenter Nonrandomized Clinical Trial
Zwolan TA, Kallogjeri D, Firszt JB, Buchman CA
Purpose
To explore speech perception and quality-of-life (QoL) effectiveness of cochlear implants (CI) in a group of adults 65 years or older compared with an optimized bilateral hearing aid (HA) condition, and to examine the improvement on the AzBio Sentence Test for Medicare beneficiaries who meet the expanded criteria of a score of 41% – 60% in the best-aided condition.
Key messages
Cochlear implantation is a safe and effective treatment for hearing loss in adults age 65+ who meet both traditional1 and expanded2 Medicare guidelines. Results show significant and meaningful improvements in speech perception and quality-of-life, without an elevated risk profile in this population.
Methods
Wick et al.
- Non-randomized controlled trial, multicenter, prospective, repeated measures design
- 13 clinical sites
- 70 subjects age 65 years and older with postlinguistic onset of bilateral moderate sloping to profound sensorineural hearing loss with an aided CNC word score of ≤40% in the ear to be implanted and ≤50% in the contralateral ear. Note that Wick et al. is a secondary analysis of subjects age ≥65yrs who are part of the larger dataset found in Buchman et al.
All subjects were experienced users of hearing aids and completed objective speech perception testing and subjective QoL surveys prior to implantation. All enrolled subjects were implanted with a CI532 electrode and used a Nucleus® 7 Sound Processor on the implanted ear and a new ReSound hearing aid on the contralateral ear. Subjects were seen by their clinicians at 1m, 3m, 6m and 12m post-activation, with endpoint measurements collected at the 6m visit. Subjects also completed a post-operative high-resolution CT scan to confirm electrode placement.
Zwolan et al.
- Non-randomized, multicenter, prospective clinical trial
- 8 clinical sites
- 34 subjects age 65+ years with bilateral moderate to profound hearing loss and best-aided pre-operative AzBio Sentence Test scores of 41-60%. Note that the current CMS criteria require a score of 40% or poorer.
The study examined speech recognition, telephone communication, hearing device benefit, health utility and quality-of-life in a group of Medicare beneficiaries. Assessments were performed pre-operatively, and at 6m and 12m post-cochlear implantation.
Results
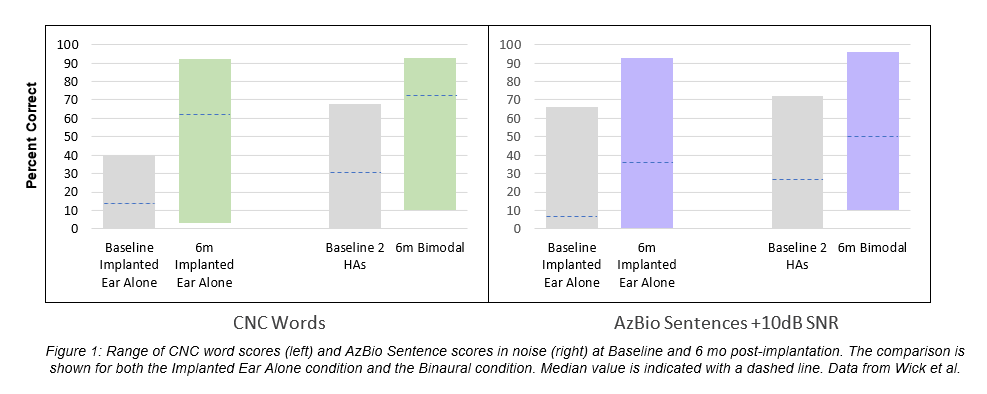
Wick and colleagues found that CIs provided meaningful improvement in speech perception and QoL in a population of 70 subjects who were age 65+ years at the time of implantation. The subjects demonstrated an estimated marginal mean (EMM) improvement in CNC words scores of 44.1% in the implanted ear alone, and 32.7% in the bimodal condition (CI+HA). Individually, 83% of subjects showed an improvement of 15% or more in the bimodal condition. On AzBio Sentences at +10dB SNR, the EMM score improved by 24.5% in the implanted ear alone and by 21.6% in the bimodal condition (Figure 1).
The Total score on the Speech, Spatial, and Qualities of Sound survey (SSQ49) improved from a baseline score of 2.04 to score 4.97 at 6 months post-CI – a difference of 2.93 points on a 10-point scale. On the Health Utilities Index (possible score range of 0-1.0), the average pre-operative hearing score was low (0.298 with bilateral HAs) and increased to 0.605 after 6 months of using a CI and HA together (change of 0.307). At this 6-month endpoint, 94% of the subjects reported that they were satisfied with their everyday listening condition, compared with only 9% of subjects who were satisfied pre-operatively when using two well-fit HAs.
In addition to the objective and subjective benefit of CI seen in this cohort, the surgery was generally well tolerated with no major adverse events within these first six months. All reported adverse events were minor, and typically associated with a CI, suggesting that this age group of recipients do not seem to present at higher risk for complication when comorbidities are appreciated and managed pre-operatively.
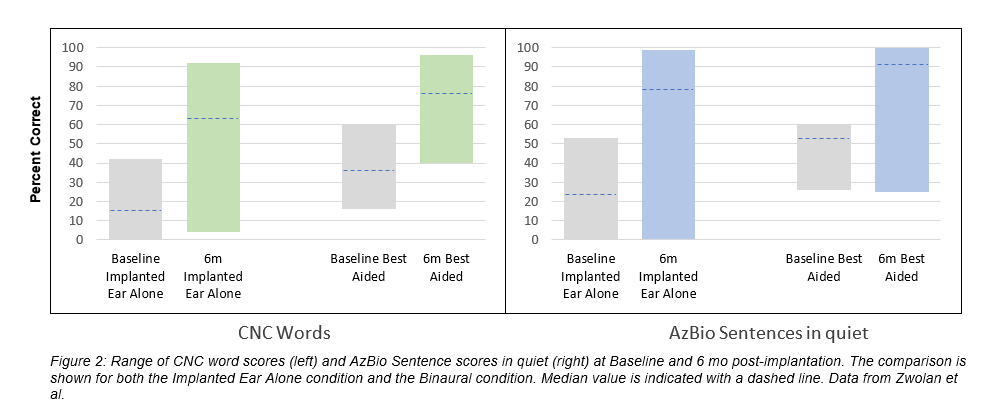
In agreement with the Wick article, Zwolan et al. reported similar speech perception benefits in a group of 31 subjects age 65+ years. The group in this study is further defined by their pre-operative scores of 41-60% on AzBio sentences which is better than the currently approved Medicare guideline. On CNC words, the EMM increased by 43% in the implanted ear alone, and by 36.5% in the best aided condition at six months post-implantation. On AzBio Sentences in quiet, the group demonstrated an EMM increase of 42.4% in the CI alone condition and 32.3% in the best-aided condition (Figure 2). The subjects’ reports of perceived hearing and health benefit also reflected significant and clinically meaningful improvement after receiving a CI.
Conclusions
The results of these two clinical trials of participants ≥ 65 years found clinically important speech understanding improvements in quiet and noise, and notable QoL and hearing satisfaction benefits when using a CI or a CI+HA versus using bilateral HAs. The advantages were seen in subjects who meet the current CMS indication for cochlear implantation, as well as in those who exceed it by as much as 20%. Complications and adverse events were neither major nor prolonged, indicating the risk/benefit profile to be acceptable for this age group. These findings suggest that cochlear implantation in older adults could be extended to those with better pre-operative speech understanding and could contribute to a healthy aging process.
To learn more subscribe to Cochlear ProNews.
References
Buchman CA, Herzog JA, McJunkin JL, et al. Assessment of Speech Understanding After Cochlear Implantation in Adult Hearing Aid Users: A Nonrandomized Controlled Trial. JAMA Otolaryngol Head Neck Surg. Published online August 27, 2020. doi:10.1001/jamaoto.2020.1584
Citation:
- Wick CC, Kallogjeri D, McJunkin JL, et al. Hearing and Quality-of-Life Outcomes After Cochlear Implantation in Adult Hearing Aid Users 65 Years or Older: A Secondary Analysis of a Nonrandomized Clinical Trial. JAMA Otolaryngol Head Neck Surg. Published online August 27, 2020. doi:10.1001/jamaoto.2020.1585
- Zwolan TA, Kallogjeri D, Firszt JB, Buchman CA. Assessment of Cochlear Implants for Adult Medicare Beneficiaries Aged 65 Years or Older Who Meet Expanded Indications of Open-Set Sentence Recognition: A Multicenter Nonrandomized Clinical Trial. JAMA Otolaryngol Head Neck Surg. Published online August 27, 2020. doi:10.1001/jamaoto.2020.2286
Authors & Affiliations:
Department of Otolaryngology–Head and Neck Surgery, Washington University School of Medicine in St Louis, St Louis, Missouri
Cameron C. Wick, MD (1)
Dorina Kallogjeri, MD, MPH (1,2)
Jonathan L. McJunkin, MD (1)
Nedim Durakovic, MD (1)
Laura K. Holden, AuD (1)
Jacques A. Herzog, MD (1)
Jill B. Firszt, PhD (1,2)
Craig A. Buchman, MD (1,2)
Statistics Editor, JAMA Otolaryngology–Head & Neck Surgery
Dorina Kallogjeri, MD, MPH (1,2)
Department of Otolaryngology-Head and Neck Surgery, Michigan Medicine, Ann Arbor
Teresa A. Zwolan, PhD (2)
This article is intended to serve as a resource for clinicians to help keep up to date with current clinical literature and is intended for professionals only. Clinical literature is based on research, which may include the experimental use of new or currently available products and technologies. Therefore, literature presented on this blog may represent use of Cochlear products that does not align with the intended use or indications approved by regulatory bodies, also known as off-label use. Cochlear does not condone any off-label use of its products, and it is not Cochlear’s intent to promote off-label use by providing this blog as a resource to clinicians.
This content is meant for professional use. If you are a consumer, please seek advice from your health professional about treatments for hearing loss. Outcomes may vary, and your health professional will advise you about the factors which could affect your outcome. Always read the instructions for use. Not all products are available in all countries. Please contact your local Cochlear representative for product information. Views expressed are those of the individual. Consult your health professional to determine if you are a candidate for Cochlear technology.
All figures are our own.
For compatibility information and devices visit www.Cochlear.com/compatibility and resound.com/compatibility. For a list of compatible ReSound hearing aids visit www.Cochlear.com/nucleus/compatibility



